
FED Method in Conservative Treatment of Chronic Pain in Adult Scoliosis.
Santos Sastre (1), J. Pedro Lapuente (2), Carlos Barrios(3).
(1) Centro de Rehabilitación y Medicina Física, Aribau 298-300, 08006 Barcelona, Spain.
(2) Centro Fisioterapeutico de Zaragoza, Maria Moliner, 50-52, 50007 Zaragoza, Spain.
(3) Instituto de Medicina del Deporte y Traumatología, General Elio 4, 46010 Valencia, Spain.
Abstract– One of the most important sequels of scoliosis in adults is pain, caused either by muscular over use and imbalance or by nerve root compression. This is very difficult sequel to treat because of the failure of the common analgesic drugs and physiotherapy treatments. We studied 30 patients with degenerative scoliosis of different etiology and Kind-Moe. There were 24 women and 6 men. Patient age ranged from 25 to 55 years old. The initial Cobb fluctuated from 25º to 65º, being 35º the average. The mean dorsal Schöber´s test at the beginning of treatment was 1.32.
The quantity of sessions of the F.E.D method were between 20 and 60, with a medium of 45 sessions. They all had case-history of NSAIDs, miorelaxing and physical therapy treatment. The final average Cobb angle was 33º and the Schöber 2.88. After the treatment only two cases required NSAIDs, miorelaxings and physiotherapy. The F.E.D. method seems to be a promising alternative for treatment of painful sequels in adult scoliosis, since in our study it was sufficiently proved the disappearance of symptomatology in the majority of cases. F.E.D. method had also a permanent effect over the time, if the patient does at home physiotherapy program. This analgesic effect, has a direct relation with the improvement we reach in the index of flexibility.
Introduction
The three main sequels of structured scoliosis in adults are, in order of importance, restrictive respiratory insufficiency, pain and deformities.
The pain in adults with scoliosis is a symptom with much worse prognosis than in non-scoliotic adults because conventional treatments (NSAIDs, muscle relaxants, analgesic physiotherapy) are much less effective, in terms of results and stability of results over time.
In the clinical setting, the authors have noted that in most patients with painful adult scoliosis there is a considerable reduction in spinal flexibility, with a Schöber back score under 2. Therefore, as the FED method had obtained an improvement in Schöber values in Scheurmann´s disease and this score is related to painful adult scoliosis, the current authors conducted a study to determine whether pain could be reduced by improving the Schöber in these patiens.
Material and Method
We studied 30 patients with degenerative scoliosis of different etiology and King-Moe. There were 24 women and 6 men. Patient age ranged from 25 to 55 years old. Mean patient age was 45 years old. The initial Cobb fluctuated from 25º to 65º, being 35º the average. The mean dorsal Schöber´s test at the beginning of treatment was 1.32, and in all of them a history of least 5 years of pain. The type of scoliosis were, King-Moe I: 13%; King-Moe II and V: 40%; King-Moe III: 20% and King-Moe IV: 27%.
Distribution based on Symtomatology we find, Occasional slight discomfort: 33%; Intermittent pain: 27%; Continuous pain not preventing ADL: 23% and Continuous pain that prevents ADL: 17%. 4 patients required some kind of analgesic treatment (NSAIDs and/or muscle relaxants and/or analgesic physiotherapy) occasionally (maximum once a month); 6 required some kind of analgesic treatment regularly (maximum twice a month); 8 required analgesic treatment regularly (4 to 5 times a month); 7 required analgesic treatment regularly (twice a week or more) and 5 required some kind of analgesic treatment daily.
The initial Schöber´s test were, 0,5 or under: 23%; 0,6 to 1,5: 40%; 1,6 t 2,5: 30% and 2,6 to 3,5: 7%. (Normal Schöber´s test: 4). The total number of sessions applied in each case ranged from 20 to 60 (mean 45). Patients received FED method treatment. It consisted of preparing the back area, using: 1. Electrotherapy and Thermotherapy for 10 minutes.
- Applying 30 minutes external corrective forces on the scoliosis curve [1][2]. These were generated by a designed, experimented and patented system (F.E.D.) [3]. This system allows the rachis to be elongated and set three-dimensionally while applying a pressure of 1 to 100 kg to the apex of the scoliosis curve, derotating and inflecting it intermittently (30 seconds of pressure and 10 of relaxation) [3][4]. FIG. 1
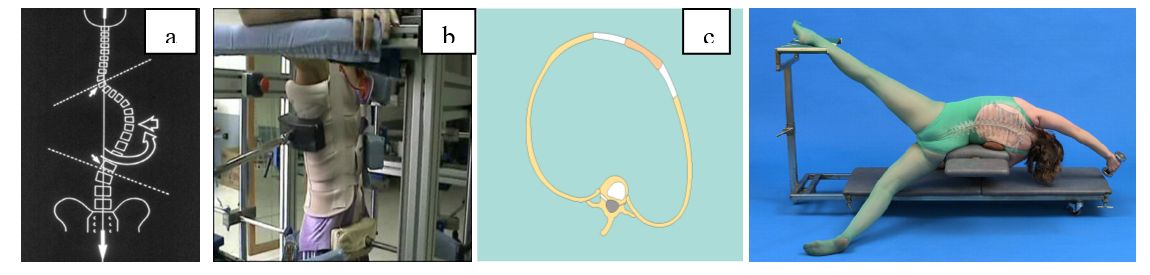
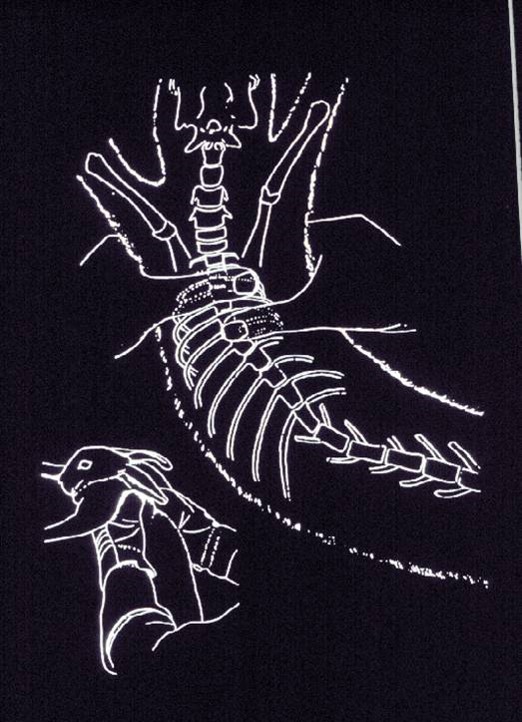
FIG.:a) Fixation, Elongation and Desrotation. b) and c) External Forces FIG. 2 Orthospinal System (OSS)
- Every session ended with 30 analytical, hypercorrective, selfcorrective and postural kinaesthetic awareness physiotherapy techniques, using an orthospinal system (OSS), kinesitherapy and PNF. FIG. 2

Clinical follow-up assessment was performed every 10 sessions and X-Ray evaluation at the beginning and the end of treatment.
Results
Treatment with the FED method achieved a significant improvement in adult scoliosis [3][4].
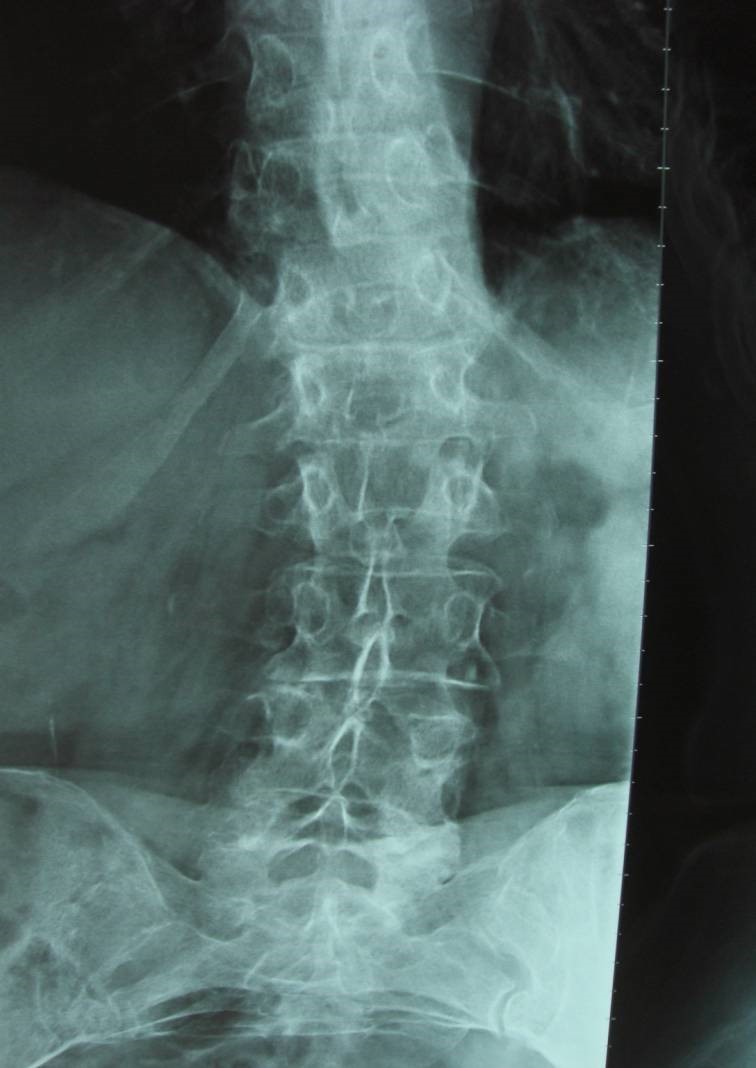
- The Cobb angle obtains a statistically significant reduction 35º to 33º, in adult patients with Risser 5 and some of then with degenerative process.FIG. 3
FIG. 3 X-Ray 1) before and 2) after 45 session FED method. Initial pain: 10 final pain: 0
- The mean dorsal Schöber´s test at the beginning of treatment was 1.32. The final Schober´s test, after the FED treatment, was 2.88.
To determine Schöber correction using FED method we compares two sampling means in a group of (2)30 patients. The mean Schöber correction in the FED group was 38.75%. The mean Schöber correction in the control group was 18.75%.
- Differences in pain before and after FED treatment. Before the treatment the 77% the scoliotic patients were symptomatic. At the end of treatment the 93% of the patients were asymptomatic. After the treatment only two cases required NSAIDs, miorelaxings and physiotherapy. We find that more flexible the spinal column is, the less pain and need for analgesia are.
Conclusions
The F.E.D. method seems to be a promising alternative for treatment of painful sequels in adult scoliosis, since in our study it was sufficiently proved the disappearance of symptomatology in the majority of cases. F.E.D. method had also a permanent effect over the time, if the patient does a home kinesiherapy program. This analgesic effect has a direct relation with the improvement we reach in the index of flexibility.
References
[1] D.L. STIWELL, and M.D. STANFORD. Structural Defomities of vertebrae Bone adaptation and Modeling in Experimental Scoliosis and Kyphosis. J. Bone Joint Surg. 44 A, 611-634, 1962.
[2] I.A.F. STOKES, H. SPENCE, D.D. ARONSSON and N. KILMER. Mechanical Modulation of Vertebral Body Growth. Spine 21, (10), 1.162-1167, 1996.
[3] J. TRESERRA, and S. SASTRE. Acción de la fisioterapia en la escoliosis experimental . Rev. Ortop. Traum., 33B.l.págs. 117-124. 1989.
[4] H.R. WEISS, I.HECKEL and C. STEPHAN. Application of passive transverse forces in the rehabilitation of spinal deformities. A randomized controlled study. Research into Spinal Deformities. Amsterdam. IOS Press.2002
Leave a reply →



{kind=link}
{kind=link}
{kind=link}
{kind=link}
It’s awesome that this article talked about the F.E.D. approach appears to be a potential alternative for treating painful sequels in adult scoliosis, as the eradication of symptomatology in the majority of patients was properly demonstrated in our study. I’m glad that you explain it thoroughly and now it makes more sense. You did a great job of explaining scoliosis.
Reply →Is there any chance this method will be available in USA? My daughter 12 was using it over the summer in Poland, and her lumbar curve went down from 45 to 33!
Reply →